
Part I
by Dr. Carver
Originally published on Zana’s Newsletter on Substack. Republished with permission.
Overview
The Washington State Department of Health is meeting again this Thursday to discuss adding the COVID-19 experimental products to the vaccine schedule for children to attend school and day care. They are being advised by a Technical Advisory Group (TAG) evaluating 9 criteria. I will be responding only to criteria 4 in this post. My colleague, Lara Gabriel RN, wrote a fantastic rebuttal to criteria 6! Since there is so much so write about criteria 4, I will complete this post in 2 parts.
Here’s a TAG summary.
• The committee is extremely pro-vaccine biased instead of pro-safety biased
• They have presented false data
• They have misrepresented data
• They have asked for a vote on criteria 6 with no relevant data for this age group
• They are deciding for 3–5-year-olds, for which there isn’t even an EUA granted by the FDA
• They are pushing this as an emergency but according to my calculation, the risk of death from Covid-19 (SARs-CoV-2) for children in Washington State aged 19 and under is 0.0007345%
Criteria 4
The TAG admits there are vaccine-related risks, but the TAG justifies these risks as acceptable due to an alleged ongoing public health emergency. They have done everything possible to inflate the risk perception of death and morbidity from COVID-19 and used every tactic to minimize the risk perception of the experimental C19 inoculations. Furthermore, no one has calculated a proper risk benefit analysis of these injections in children.
I would like to do a risk comparison of the COVID-19 virus versus the C19 injections in children regarding the risk of death, myocarditis, and multisystem inflammatory syndrome in children (MIS-C) or (MIS-V) if vaccine associated. Since this could result in a very long post, I’m going to address the relative risk of death and give some information from VAERS regarding reports of death, myocarditis and pericarditis, and MIS-V. I will come back to this this to finish in part II.
Relative Risk Comparison
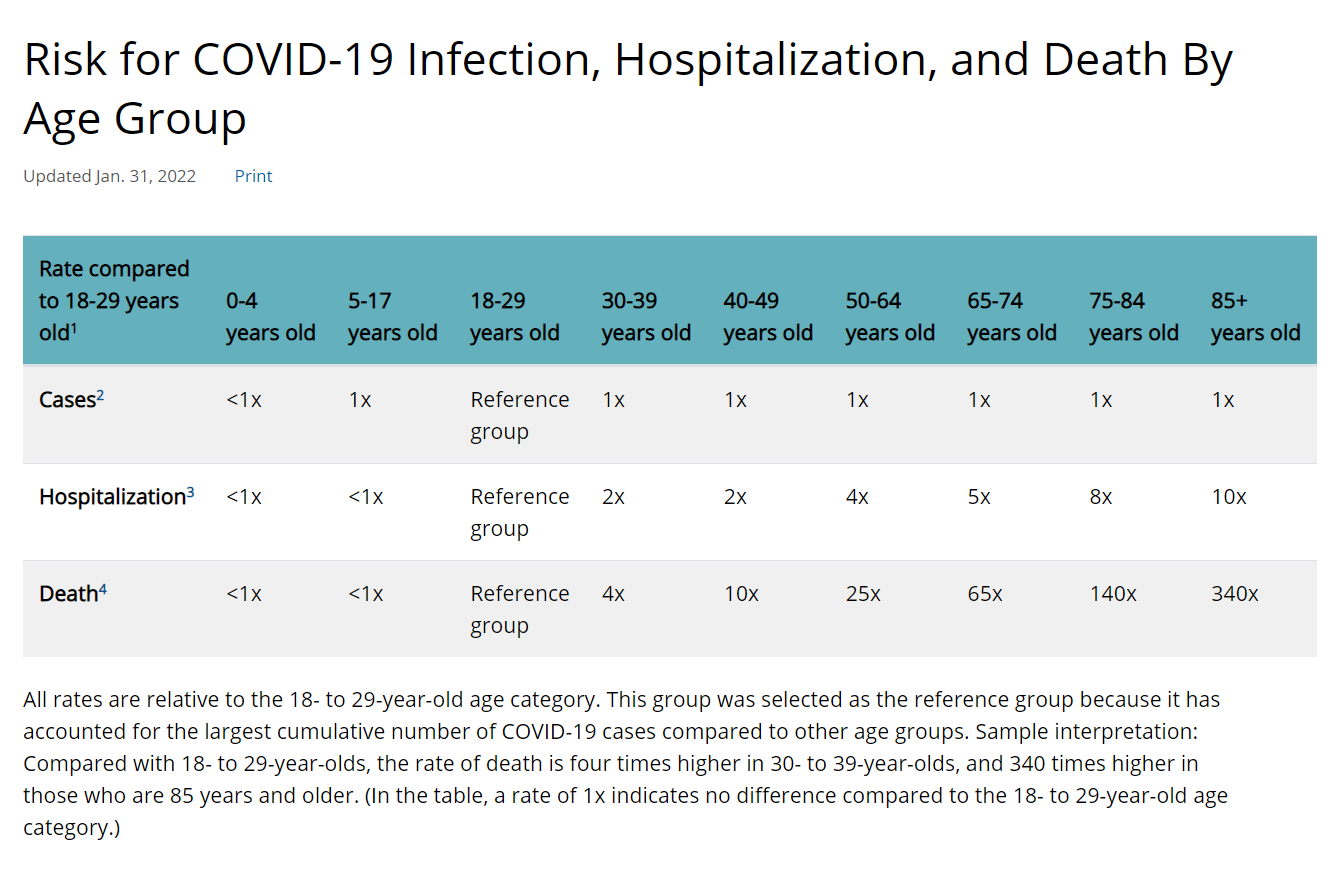
In WA state there have been 13 deaths in children, which means that the death rate from Covid-19 for children in WA state aged 19 and under is 0.0007345%. The CDC continues to acknowledge that the elderly and those with, on average 4 co-morbidities, have the greatest risk of morbidity and mortality from COVID-19. Even the TAG presenters acknowledged that Omicron is less likely to cause severe morbidity and mortality than other variants.
Risk of the C19 Injections
VAERS Overview
During the WSBOH meetings it was stated that the vaccine adverse events reporting system (VAERS) is passive and unreliable. They stated anyone can make a report. This is misleading in several ways because most healthcare providers do not know that reports are supposed to made for any adverse event after a vaccination. This does not imply causality but instead can give important safety signals that can be researched further with medical charts, lab reports, test results, pathology, and autopsy findings as well as surveys and correlating the results with other reporting systems.
It is a federal offense to falsify a report. It’s worth mentioning that 85% of reports are completed by healthcare professionals and 15% are filled out by the patient or a close relative. The reports are time consuming, and a considerable amount of medical knowledge is required. Because they are time consuming, many healthcare professionals do not have time to fill out these reports and the ones who make time are often reprimanded or fired.
Several studies have calculated the underreporting factor for these reports, including the Harvard Pilgrim study, Dr. Jessica Rose, and Steve Kirsch. The underreporting factor that Dr. Rose found is the most conservative and was calculated as 31. This means that you need to multiply the adverse event number in each category by 31 to get a more accurate picture of the true number of events.
Also, in the TAG group, the V-Safe phone app was promoted as being more reliable. From firsthand vaccine damaged individuals, these apps are limited to multiple choice entries; not all adverse events are recorded and it is completely voluntary. Some vaccine damaged individuals were denied access to the app when they had adverse events. This is the reason why their serious adverse event list is incredibly short while the mild adverse event list is relatively long. The vaccine safety datalink (VSD) is managed by the CDC with nine healthcare organizations, but the information is not open to the public. I emailed to see if there was any opportunity for an independent scientist to access the data and their email response was a flat “NO.” This is consistent with the CDC hiding safety data and the FDA and Pfizer fighting in court to delay the release of the safety data.
CDC contractors do investigate and remove any duplicate reports, but there are reports removed without any explanation that are not duplicate reports. Updates are collected but the reports are not updated for the public.
Please see Rose J. 2021. Critical appraisal of VAERS Pharmacovigilance: Is the U.S. vaccine adverse events reporting system (VAERS) a functioning pharmacovigilance system? Science, Public Policy, and the Law; Clinical and Translational Research 3:100-129. Accessed 11/10/2021, https://resistance-mondiale.com/wp-content/uploads/2021/11/adf864_0490c898f7514df4b6fbc5935da07322.pdf for further details.
What Does VAERS Show?
In VAERS there have been 34,223 adverse events in children reported through February 11, 2022.
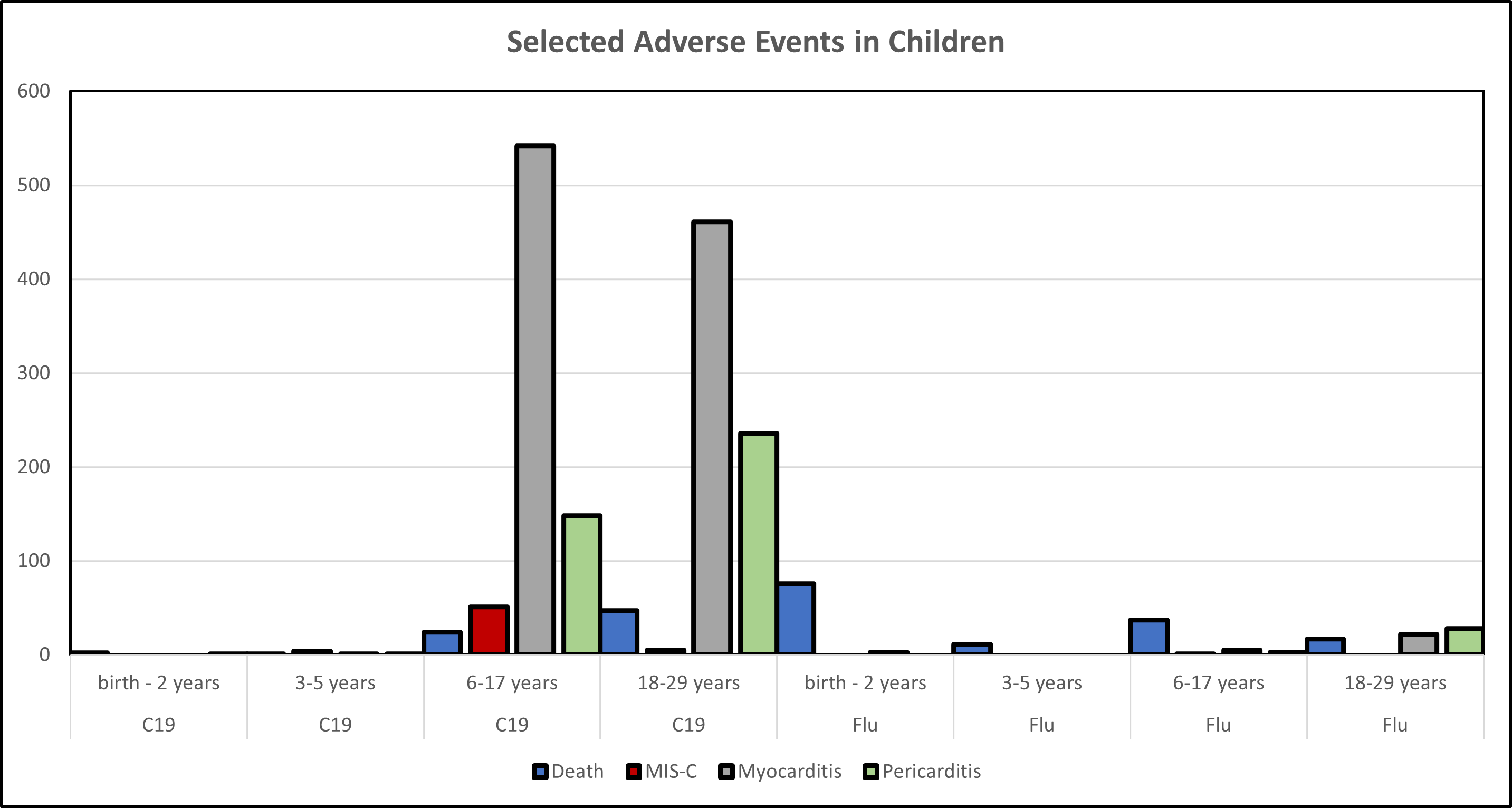
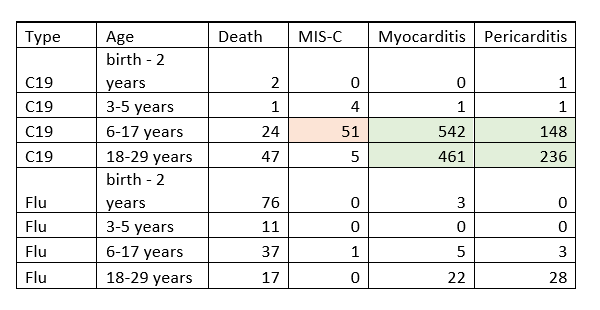
Here are the raw numbers from the VAERS Wonder System on 2/22/2022. Remember to get an accurate count you would need to multiple each category by the underreporting factor (URF) of 31.
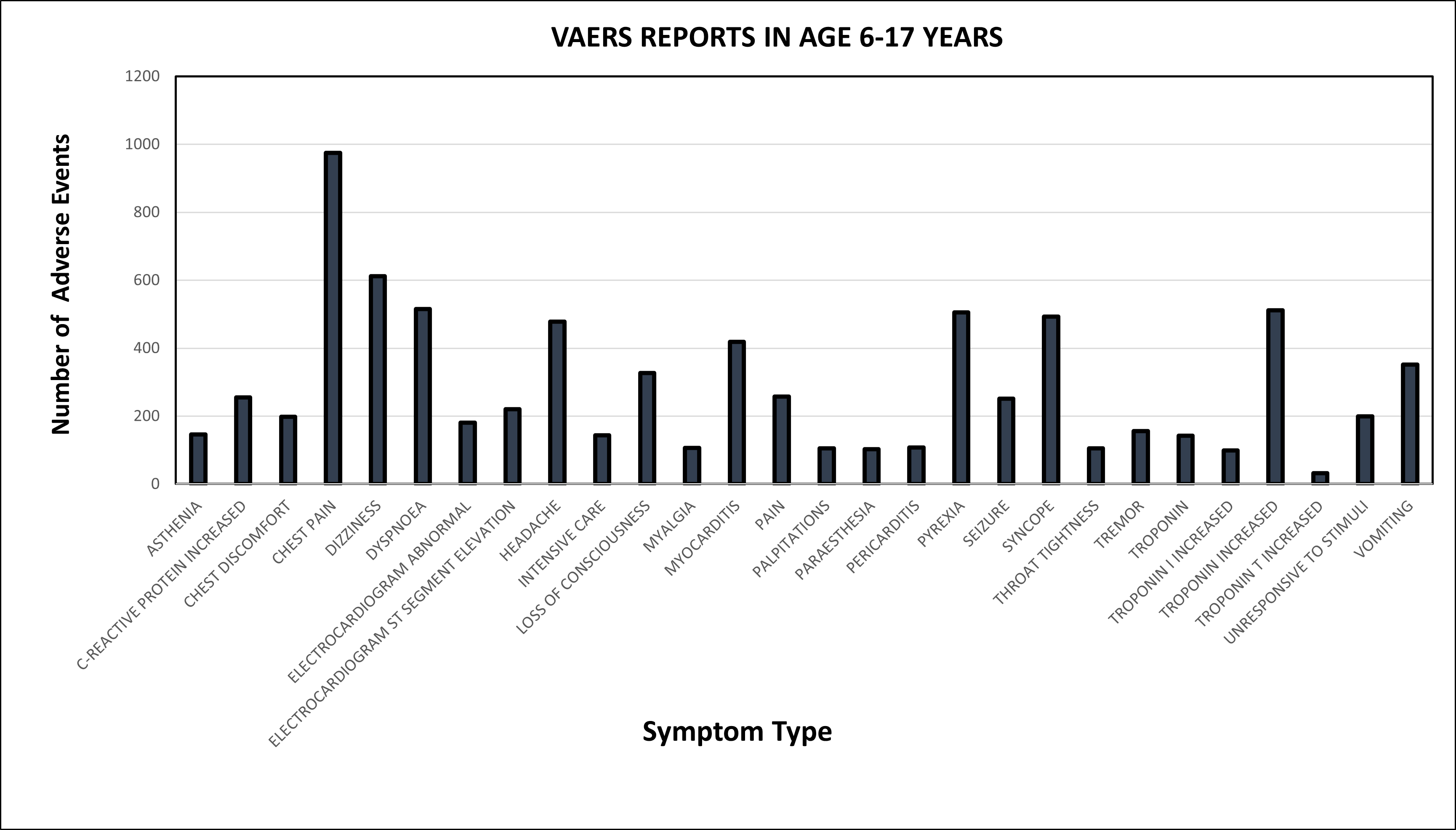
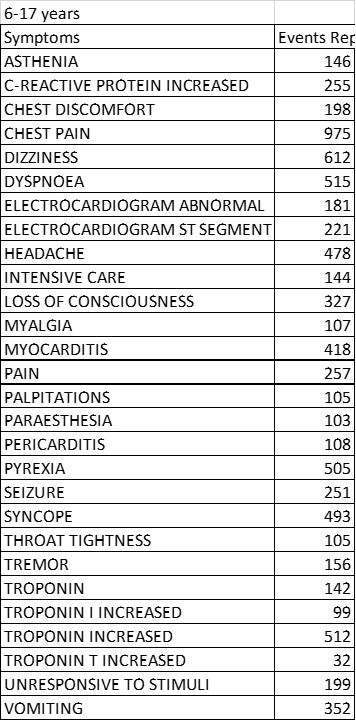
This is where I need to point out that the elevated troponin levels indicate cardiac damage. When you combine this finding with chest pain and the relatively high numbers of myo-pericarditis cases, especially in boys after the second injection, it’s clear that these inoculations are not as benign as they would have you think. I will delve into this deeper in part 2 but I want to leave you with one last thought.
There is a high amount of consistency between the reports in VAERS, the FDA’s list of adverse events of concern, medical reports, lab tests, pathology reports, and autopsy findings. There is also a very close association between age-specific vaccine role-out dates and age-specific increases in excess mortality. Lastly, even morticians and funeral directors are noticing elevated deaths from blood clots, strokes, and cardiac failure. The weight of evidence clearly supports that these inoculations have considerable risk. In a future post, I will use the Bradford Hill criteria to show a causal association.
Summary
How can the TAG continue to downplay the risk of vaccine associated myocarditis, elevated troponin levels, elevated CRP, chest pain, elevated D-dimer levels, MIS-V, seizures, and other vaccine related adverse events by stating that COVID-19 in children is an emergency? What about the lack of studies in children such as genotoxicity, carcinogenicity, reproductive toxicity, pharmacokinetics, biodistribution, cardiac toxicity, and vaccine-associated enhanced respiratory disease (VAERD)? Why would anyone think it’s okay to use children in a population-level experiment without any understanding of the long-term health consequences of the C-19 vaccines in children?
References
- Lara Gabriel RN WSBOH Criteria #6 Rebuttal
- https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html
- https://ofm.wa.gov/washington-data-research/statewide-data/washington-trends/population-changes/distribution-washington-population-age-and-gender
- https://unityprojectonline.com/say-no-to-sb-866-and-say-no-to-adding-the-c-19-tax-to-sb-871/
- https://openvaers.com/covid-data/child-reports
- WSBOH: Criteria 5 Rebuttal
- CDC Has Finally Been Caught by Legacy Media – And Their Stated Reasons Why are Really, Really Bad
- Autopsies in VAERS
- How rare are vaccine side effects? Not very rare at all.
- https://denisrancourt.ca/entries.php?id=109&name=2022_02_09_nature_of_the_toxicity_of_the_covid_19_vaccines_in_the_usa
- WHO’S MORE AT RISK FROM THE C-19 INJECTIONS?
- Bhakdi/Burkhardt pathology results show 93% of people who died after being vaccinated were killed by the vaccine
- https://doctors4covidethics.org/wp-content/uploads/2021/12/end-covax.pdf
- https://www.canadiancovidcarealliance.org/wp-content/uploads/2022/02/Scientific-Review-Dispelling-the-Myth-of-a-Pandemic-of-the-Unvaccinated.pdf
- https://www.canadiancovidcarealliance.org/wp-content/uploads/2021/12/The-COVID-19-Inoculations-More-Harm-Than-Good-REV-Dec-16-2021.pdf
- 1. Lazarus R., et al. (2010). Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS) Accessed 10/25/2021, https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
- Kirsch S., et al. (2021). Estimating the number of COVID vaccine deaths in America. https://docs.google.com/document/d/1stq2nHFjAcMHhxJhWiXa33wl6x0Ga1qdIxodZnFixRw/edit#
- Rose J. 2021. Critical appraisal of VAERS Pharmacovigilance: Is the U.S. vaccine adverse events reporting system (VAERS) a functioning pharmacovigilance system? Science, Public Policy, and the Law; Clinical and Translational Research 3:100-129. Accessed 11/10/2021, https://resistance-mondiale.com/wpontent/uploads/2021/11/adf864_0490c898f7514df4b6fbc5935da07322.pdf
- Lyons-Weiler J. 2021. Five Studies on mRNA Vaccine Spike Protein Pathogenicity. Share with Your Doctor. Ignore the “Fact Checker” Opinion Web Sites. Here’s a Collection of Resources on Spike Protein Pathogenicity for Your Use. Add Your Own in the Comments.
- Kostoff RN, Calina D, Kanduc D, Briggs MB, Vlachoyiannopoulos P, Svistunov AA, Tsatsakis A. 2021. Why are we vaccinating children against COVID-19? Toxicology reports 8:1665-1684.Lai CC, Chen IT, Chao CM, Lee PI, Ko WC, Hsueh PR. 2021. COVID-19 vaccines: concerns beyond protective efficacy and safety. Expert Rev Vaccines 20(8):1013-1025.
- Kirsch S. 2021. New VAERS analysis reveals hundreds of serious adverse events that the CDC and FDA never told us about. They missed hundreds of serious adverse events that are more elevated than myocarditis. A new VAERS analysis done by Albert Benavides blows the doors off the “safe and effective” narrative.
- Nonclinical Evaluation Report: BNT162b2 [mRNA] COVID-19 vaccine (COMIRNATY ™) 2021. Submission No: PM-2020-05461-1-2 Sponsor: Pfizer Australia Pty Ltd. https://www.tga.gov.au/sites/default/files/foi-2389-06.pdf
- Rose J. 2021. “The shortcoming of the repeat dose toxicity study design should not preclude approval of the vaccine.” https://jessicar.substack.com/p/the-shortcoming-of-the-repeat-dose
- Oehler A. 2021. Does mRNA in Jabs Really Produce S Spike from SARS-CoV02? The evidence points to something else altogether.
- https://sboh.wa.gov/meetings/meeting-information
- https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-11-2-3/05-COVID-Shimabukuro-508.pdf
- https://wonder.cdc.gov/controller/datarequest/D8;jsessionid=184249C20F67C63657F8B6BA69E4
- https://wonder.cdc.gov/vaers.html
- https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf