
HPV
A study published on June 11, 2018, shows a reduced number of conceptions for 25-29 year old women who received HPV vaccinations.
- Gayle DeLong(2018) A lowered probability of pregnancy in females in the USA aged 25–29 who received a human papillomavirus vaccine injection, Journal of Toxicology and Environmental Health, Part A, 81:14, 661-674, DOI: 1080/15287394.2018.1477640
The FDA was also aware of autoimmune disorders that appeared during clinical trials. The FDA approves all language of inserts. Read the following carefully.
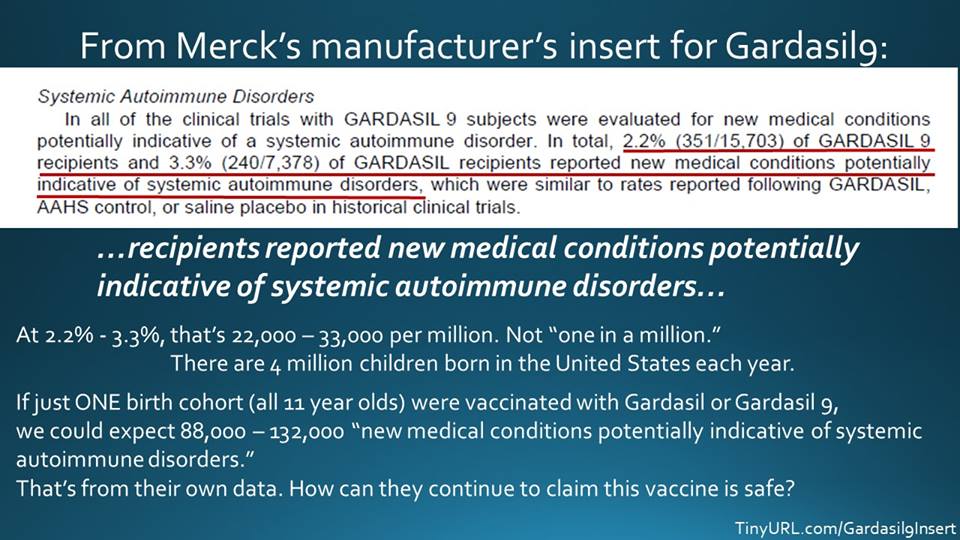
Merck’s Gardasil 9 insert (excerpt above) mentions rates of new systemic autoimmune disorder in subjects and claims they were similar to “saline placebo” rates in historical clinical trials for Gardasil. Or do they? Look carefully at the actual language on the insert — “. . . which were similar to rates reported following GARDASIL, AAHS control, or saline placebo . . .” (emphasis added) . The word “or” was very carefully chosen for legal purposes by Merck and is extremely deceptive.
The clinical trials included just one small saline placebo group and these results were rolled into aluminum adjuvant “AAHS” groups. Notably, none of those in the saline saline group died, and NONE OF THE SUBJECTS IN THE SALINE PLACEBO GROUP DEVELOPED A NEW AUTOIMMUNE DISORDER. In the other clinical trials, out of 29,000 subjects, there were 40 deaths – evenly split between the Gardasil group and the AAHS (a potent aluminum adjuvant) group. The death rate was 1 in 733; 1 in 718 if you subtract the saline placebo group. SEE CRITICAL DATA ON ALUMINUM ADJUVANTS.
ICAN — The Informed Consent Action Network — is taking action on the deceptive label (click image for link to full letter):
Excellent Investigative Journalism about HPV clinical trials in Slate.com article: https://slate.com/health-and-science/2017/12/flaws-in-the-clinical-trials-for-gardasil-made-it-harder-to-properly-assess-safety.html
“An eight-month investigation by Slate found the major Gardasil trials were flawed from the outset, however, and that regulators allowed unreliable methods to be used to test the vaccine’s safety. While these flaws do not mean Gardasil caused the rare crippling illnesses reported by the media, they are troubling. Public health officials use trials like these both to determine safety and, as evidenced by Merck’s statement above, to reassure the public when concerns like the ones about Gardasil arise. A flawed study design can complicate both tasks.”
About HPV
Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States. There are more than 200 strains (and counting). In the vast majority of cases it causes no health problems and completely clears on its own.
An Independent Journalist writes about the current state of HPV vaccine around the world: Are We Seeing a Global HPV Vaccine Fraud Implosion?
“The US has paid out over $6 million for damages from the HPV vaccine. The US Vaccine Adverse Event Reporting System (VAERS), thought to catch less than one percent of all reactions, has recorded nearly 52,000 adverse reactions from the shot.”
Why HPV vaccines are unnecessary
- More than 90% of HPV infections clear on their own
- Regular pap smears are still needed and are very effective at preventing cervical cancer by early intervention
- Precancerous lesions are curable
- Maintaining a healthy diet and lifestyle further reduces risk of HPV complications
- https://report.nih.gov/nihfactsheets/viewfactsheet.aspx?csid=76
Why HPV vaccine impact on cancer unknown
- It takes on average 30 years for cancer to develop in the rare cases when HPV infection does lead to cancer. The impact of vaccination programs is not yet known.
- Strain replacement has been found to occur. There are more than 200 strains of HPV. While the current Gardasil9 vaccine protects against what are thought to be the strains leading to the most cancer, It is not known what impact other strains may have on cancer rates or on other health conditions. “The number of studies that show that partial immunization via available HPV (human papillomavirus) vaccines is not only insufficient at reducing overall HPV infection rates; the vaccines actually cause rarer, more lethal types of HPV to sweep in and the net effect could be devastating increases in HPV-related cancers.” Dr. James Lyons-Weiler.
-
Cervical cancers after human papillomavirus vaccination. “CONCLUSION: Long-term follow-up data are needed to evaluate the prophylactic effectiveness of the current HPV vaccine. These cases could represent non-vaccine-related HPV infections. Young women must be thoroughly counseled about the efficacy and limitations of the vaccine and about continuing lifelong.” PMID 19155953
-
Endocervical Carcinogenesis and HPV Vaccination: An Occasional Circumstance or a Gap in the Chain? “In conclusion, this case report highlights the need for diagnostic surveillance regarding HPV-related cervical cancer even after vaccination.” PMID 28116194
-
Expression of p16INK4A in Cervical Precancerous Lesions unlikely to be preventable by HPV Vaccines “Lesions that may develop due to HR-HPV genotypes not included in HPV vaccines are likely to have similar malignant potential, suggesting that well developed screening programs combined with non-vaccine based approaches may be needed to manage the residual risk of developing CC in the post-vaccination era.”PMID: 27479745
Why the science on HPV vaccination is not settled
New July 2017:
Human papilloma virus and lupus: the virus, the vaccine and the disease.
“We review clinical, epidemiological and molecular data suggesting involvement of HPV infection in the pathogenesis of SLE. We suggest that these findings may justify the development of new HPV vaccines containing viral peptides that bear no homology to the human proteome, in order to avoid possible adverse immune cross-reactivity.” PMID:28394823
Serious adverse events after HPV vaccination: a critical review of randomized trials and post-marketing case series.
Abstract
“This article critically reviews HPV vaccine serious adverse events described in pre-licensure randomized trials and in post-marketing case series. HPV vaccine randomized trials were identified in PubMed. Safety data were extracted. Post-marketing case series describing HPV immunization adverse events were reviewed. Most HPV vaccine randomized trials did not use inert placebo in the control group. Two of the largest randomized trials found significantly more severe adverse events in the tested HPV vaccine arm of the study. Compared to 2871 women receiving aluminum placebo, the group of 2881 women injected with the bivalent HPV vaccine had more deaths on follow-up (14 vs. 3, p = 0.012). Compared to 7078 girls injected with the 4-valent HPV vaccine, 7071 girls receiving the 9-valent dose had more serious systemic adverse events (3.3 vs. 2.6%, p = 0.01). For the 9-valent dose, our calculated number needed to seriously harm is 140 (95% CI, 79-653). The number needed to vaccinate is 1757 (95% CI, 131 to infinity). Practically, none of the serious adverse events occurring in any arm of both studies were judged to be vaccine-related. Pre-clinical trials, post-marketing case series, and the global drug adverse reaction database (VigiBase) describe similar post-HPV immunization symptom clusters. Two of the largest randomized HPV vaccine trials unveiled more severe adverse events in the tested HPV vaccine arm of the study. Nine-valent HPV vaccine has a worrisome number needed to vaccinate/number needed to harm quotient. Pre-clinical trials and post-marketing case series describe similar post-HPV immunization symptoms.” PMID: 28730271
Article: New Study: Vaccine Manufacturers and FDA Regulators Used Statistical Gimmicks to Hide Risks of HPV Vaccines by Robert Kennedy, Jr. World Mercury Project
“When it came time for Merck to report on the occurrence of more serious reactions, “Systemic Adverse Reactions” and “Systemic Autoimmune Disorders,” for example, the company scientists switched to a very different format. In these tables, the third column that reported results for the saline placebo recipients disappears. Instead, Merck combined the groups receiving the spiked aluminum placebo into a single column with the group receiving the genuine saline placebo (see example below). The merger of the two control groups makes it impossible to compare results for Gardasil versus the saline placebo or the aluminum placebo versus the saline placebo. In this way, Merck’s researchers obliterated any hope of creating a meaningful safety comparison.”
Excerpt from: NVIC
“Using the MedAlerts search engine, as of Sept. 30, 2015, there were a total of 37,474 vaccine reaction reports made to the federal Vaccine Adverse Events Reporting System (VAERS) associated with Gardasil vaccinations, including 209 deaths. There were a total of 3,119 vaccine adverse reaction reports made to VAERS associated with Cervarix vaccinations, including 16 deaths. (Merck’s Gardasil vaccine, which was the first HPV vaccine licensed in the U.S., has the majority of the HPV vaccine market in the U.S.).”
- Serious adverse events after HPV vaccination: a critical review of randomized trials and post-marketing case series. “Abstract: This article critically reviews HPV vaccine serious adverse events described in pre-licensure randomized trials and in post-marketing case series. HPV vaccine randomized trials were identified in PubMed. Safety data were extracted. Post-marketing case series describing HPV immunization adverse events were reviewed. Most HPV vaccine randomized trials did not use inert placebo in the control group. Two of the largest randomized trials found significantly more severe adverse events in the tested HPV vaccine arm of the study. Compared to 2871 women receiving aluminum placebo, the group of 2881 women injected with the bivalent HPV vaccine had more deaths on follow-up (14 vs. 3, p = 0.012). Compared to 7078 girls injected with the 4-valent HPV vaccine, 7071 girls receiving the 9-valent dose had more serious systemic adverse events (3.3 vs. 2.6%, p = 0.01). For the 9-valent dose, our calculated numberhttps://www.informedchoicewa.org/wp-admin/post.php?post=903&action=edit needed to seriously harm is 140 (95% CI, 796-53). The number needed to vaccinate is 1757 (95% CI, 131 to infinity). Practically, none of the serious adverse events occurring in any arm of both studies were judged to be vaccine-related. Pre-clinical trials, post-marketing case series, and the global drug adverse reaction database (VigiBase) describe similar post-HPV immunization symptom clusters. Two of the largest randomized HPV vaccine trials unveiled more severe adverse events in the tested HPV vaccine arm of the study. Nine-valent HPV vaccine has a worrisome number needed to vaccinate/number needed to harm quotient. Pre-clinical trials and post-marketing case series describe similar post-HPV immunization symptoms.” PMID:28730271
- Vaccine-related serious adverse events might have been under-recognized in the pivotal HPV vaccine randomized trial. PMID:28204892
- Incidence rates of Guillain Barré (GBS), chronic fatigue/systemic exertion intolerance disease (CFS/SEID) and postural orthostatic tachycardia syndrome (POTS) prior to introduction of human papilloma virus (HPV) vaccination among adolescent girls in Finland, 2002-2012. PMID:28720463
- What do we know about the safety of the HPV vaccines? “However, there are several unresolved issues related to potentially serious harms of the vaccine. In its handling of this issue, the European Medicines Agency has not lived up to its role.”
- Human Papillomavirus Vaccine and Postural Orthostatic Tachycardia Syndrome: A Review of Current Literature. PMID:28689455
- Gardasil Researcher Speaks out. http://www.cbsnews.com/news/gardasil-researcher-speaks-out/
-
Gardasil Syndrome. http://gardasilsyndrome.com/#abstract
-
Premature Ovarian Failure. https://www.acpeds.org/the-college-speaks/position-statements/health-issues/new-concerns-about-the-human-papillomavirus-vaccine
-
Recurrent optic neuritis and neuromyelitis optica-IgG following first and second human papillomavirus vaccinations. “Demyelinating disorders within months following HPV innoculation have been reported, but the causal link between HPV vaccination and the onset of demyelinating disorders have not been certain. We report a case of neuromyelitis optica spectrum disorder (NMOSD) that was noteworthy because optic neuritis (ON) occurred in a very close temporal association with both the first and second HPV vaccinations, which might suggest an association between HPV vaccination and the development of NMO-IgG and recurrent ON. This emphasizes the necessity for continuing surveillance for adverse events after HPV vaccination. “PMID 27046292
- Neuromyelitis optica may be triggered by HPV vaccination
-
Lessons Learned in Japan http://ijme.in/articles/lessons-learnt-in-japan-from-adverse-reactions-to-the-hpv-vaccine-a-medical-ethics-perspective/?galley=html
-
Compensation for HPV vaccine injury https://ecf.cofc.uscourts.gov/cgi-bin/show_public_doc?2012vv0630-164-0
-
http://sanevax.org/wp-content/uploads/2015/11/Gomez-v-USDOH-expert-report.pdf
-
Gardasil 9: Each 0.5-mL dose of the vaccine also contains approximately 500 mcg of aluminum (provided as AAHS), 9.56 mg of sodium chloride, 0.78 mg of L-histidine, 50 mcg of polysorbate 80, 35 mcg of sodium borate, <7 mcg yeast protein, and water for injection.
-
Gardasil 9 testing was highly inadequate. Insert. FDA HPV page. There were no saline placebo clinical trials. The excerpt below reveals only comparison studies were done. The clinical trials for the original Gardasil included just one, small saline placebo group and these results were rolled into aluminum placebo groups. See PMID: 28730271
Excerpt from FDA on HPV Clinical Trials:
2.4.1 Clinical Trials with GARDASIL 9
GARDASIL 9 was studied in 6 clinical trials:
Study V503-001was a Phase 2b/3 efficacy study that enrolled 15,457 women 16through 26 years of age and randomized to receive GARDASIL 9 (low-dose, mid-dose, high-dose) or GARDASIL (comparator). The optimal dose for further investigation was defined as the “mid-dose.” This study demonstrated efficacy of 96.7% in terms of prevention of combined genital lesions (CIN2+, VIN2+, orVaIN2+) attributed to the 5 additional HPV types not present in GARDASIL.
Study V503-002was an– immunobridging study linking clinical efficacy obtained from Study V503-001 to 955 children 9 through 15 years of age. Evaluation of clinical efficacy was not feasible because performing genital examination in this population in the absence of the primary endpoint was not justifiable. Non-inferiority was demonstrated for all 9 vaccine HPV types, and lot consistency criteria were also met for the 9 vaccine HPV types.
Study V503-009 was an additional immunological bridging study (not conducted under IND) in 600 females 9 through 15 years of age which demonstrated non-inferior GMT ratios for HPV types 6, 11, 16, and 18 between GARDASIL 9 and GARDASIL
There were 3 studies evaluating vaccine coadministration: V503-005– assessment of potential interference of Gardasil 9 with concomitant Menactra and Adacel inc hildren 11 through 15 years of age V503-006-safety and immunogenicity study of Gardasil 9 in subjects previously vaccinated with the HPV vaccine V503-007-concomitant administration study with a non-U.S.-licensed vaccine (Repevax); provided safety data for GARDASIL 9i n adolescents11 through 15 years of age
Pharmaceutical Companies’ Role in State Vaccination Policymaking: The Case of HPV
