
To the Oregon Medical Board: Kathleen Harder MD, Saurabh Gupta MD, Erin Cramer PA-C, Robert M. Cahn MD, James K. Lace MD, Charlotte Lin MD, Pattie Louie PHD, Jennifer L. Lyons MD, Ali Mageehon PHD, Chere Pereira, Christoffer Poulsen DO, Andrew Schink DPM, Jill Shaw DO
On November 22, 2020, a peer-reviewed study was published in the International Journal of Environmental Research and Public Health. Titled “Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination,” the study looked at the health outcomes of children born into Dr. Paul Thomas’s pediatric practice in Portland, Oregon in which Fully Informed Consent and Personalized Medicine are the foundations of care. The study data reveal that the less children are exposed to vaccines, the healthier they are.
Pediatric vaccines are designed to do one thing—prevent a child from experiencing symptoms if exposed to a targeted virus or bacteria. That’s it. Vaccines do not provide any essential nutrients; they do not provide any of the buildings blocks of health. Vaccines are designed for symptom-avoidance from transient infections, period.
Is symptom-avoidance through vaccine exposure leading to healthier children? Does exposure to the ingredients in vaccine products on the CDC’s pediatric schedule lead to healthier children?
Is symptom-avoidance through vaccine exposure leading to healthier children?
Does exposure to the ingredients in vaccine products on the CDC’s pediatric schedule lead to healthier children?
The CDC has steadfastly refused to do any sort of study designed to answer these questions. But now we have Dr. Paul’s well-designed and executed study that posed these very questions, and we have an answer.
No.
Exposing children to vaccine products in order to avoid symptoms of transient infections does not lead to better overall health outcomes. The opposite is true.
And what was the reaction of Public Health officials in the United States to this news? Silence, as usual, from Health & Human Services (HHS), the federal agency tasked with monitoring vaccine safety. And silence from the Center for Disease Control (CDC), the federal agency that keeps adding vaccines to the pediatric schedule in the absence of long- term safety studies. HHS and CDC don’t dare acknowledge the study because they would have to admit their reckless policies must change.
And in Oregon? You, the Oregon Medical Board (OMB) called an emergency meeting on December 3, 2020. You did not meet to discuss how the study findings should be used to guide other Oregon doctors in improving health outcomes of children in their practices. Instead, you met to suspend the medical license of the doctor who co-authored the study, the doctor whose practice, Integrative Pediatrics, has possibly the lowest rate of chronic childhood disorders in the country: Paul Thomas, MD.
Perhaps the most egregious aspect of your retaliatory move was that you had demanded that Dr. Paul provide data showing that the unvaccinated patients in his practice were not less healthy than the vaccinated. He provided that data in his published study. According to the study’s co-author, Dr. James Lyons-Weiler of The Institute for Pure and Applied Knowledge,
“The Oregon Medical Board has not only declared war on actual ethical medical practice. In my view, they have declared war on objective science.”
A few other independent studies have been done that also conclude increased vaccine exposure leads to poorer health outcomes, but Dr. Paul Thomas’s and James Lyons-Weiler’s study is the strongest yet.
In your suspension order, OMB, you stated that you had the “statutory duty under ORS chapter 677 to protect the public and to exercise general supervision over the practice of medicine.”
But you completely misunderstand what that duty means. The duty to “protect the public and to exercise general supervision” is a high-level and broad authority set at the population level and does not include stepping into the legal or medical decisions of individuals nor into the patient-doctor relationship.
In fact, in making false accusations against Dr. Paul (discussed below), you have maliciously attempted to condemn Dr. Paul for simply carrying out his legal duty to act as a “Learned Intermediary,” providing the opportunity that he is legally and ethically required to provide, for fully informed consent on the subject of vaccination. Informed consent is not a fait accompli. Patients and their guardians have the legal right to decline any and all vaccines.
In fact, in not ensuring that all medical doctors are acting as “Learned Intermediaries” for their young patients, in attempting to say that “informed consent” means that all patients must be given all vaccines on the CDC schedule, you are mangling the very meaning and protection afforded by the noble and longstanding principle of Informed Consent.
Furthermore, by exerting pressure for doctors to treat all children the same regardless of individual circumstances, you are causing grave harm to the children in the state beyond ignoring their legal, ethical, and medical-due-diligence rights to choose some, all, or none of the vaccines recommended by CDC. If your goal is to vaccinate 100% of Oregon’s children according to the full and ever-growing CDC schedule, then your goal is to treat any child incapable of tolerating that schedule as acceptable collateral damage, unworthy of protection.
If your goal is to vaccinate 100% of Oregon’s children according to the full and ever-growing CDC schedule, then your goal is to treat any child incapable of tolerating that schedule as acceptable collateral damage, unworthy of protection.
And by measuring a physician’s competence based on the number of pharmaceutical products he prescribes rather than the health of his patients, you have shone a glaring spotlight on what is so very wrong with our entire current medical system today. Medicine in the U.S. has been captured through the use of built-in mechanisms for incentivizing pharmaceutical “standards of care” rather than rewarding good health outcomes.
In your charges against Dr. Paul, you, the OMB, refer to the CDC’s “Recommended Child and Adolescent Immunization Schedule for ages 18 years or younger, United States, 2020” and say that vaccine products make certain disease “preventable.” You also state that the “schedule has been relied upon for many years, is updated periodically, and is widely accepted as authoritative in the medical community.”
Our medical system, our children, are suffering because of such broad and sweeping marketing statements that have no backing in science. Consider this:
“Recommended” — the CDC provides recommendations to serve as a guide — they are neither mandates nor prescriptions to be carried out at the individual level. Doctors that attempt to vaccinate all children under their care exactly the same, by strictly following the CDC Guideline recommendations, are failing to do their legal duty to act as Learned Intermediaries, failing to personalize care to each patient based on their genetic, family and individual health history, putting them at risk of avoidable harm, and failing to provide the opportunity for fully informed consent to parents.
“Preventable” — the vaccine products on the market today attempt to prevent the symptoms of disease; they cannot be described as completely effective at preventing either infection, transmission, or disease. Some vaccines, such as the pertussis and diphtheria vaccines in the DTaP, are not even designed to prevent infection or transmission. Outbreaks of vaccine-targeted infections are occurring in fully vaccinated populations, including measles and mumps, and transmission from fully vaccinated individuals to those who are susceptible to infection is occurring.
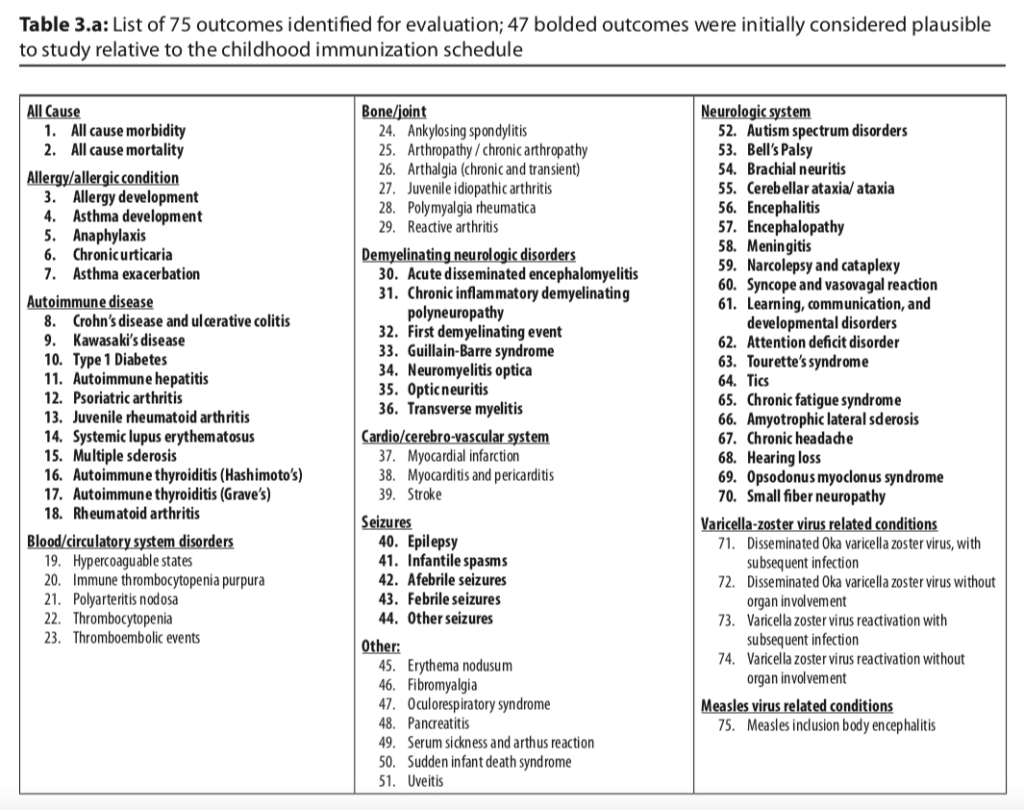
“Updated” — the CDC updates their schedule to add vaccinations, but they have never performed a single safety study on the impact of the child being exposed to the full schedule comparing fully vaccinated to fully-not vaccinated children. Because of growing public concern and anger regarding this, the CDC actually commissioned a White Paper, published in 2015, which spelled out the many plausible health problems which have been reported regarding exposure to the full CDC schedule—but which have not been adequately studied. In this white paper, it was proposed that alternative vaccine schedules be studied to compare outcomes. Far from condemning the use of alternative schedules, the CDC asked if children on those schedules fared better. Does this conflict with our statement above that the CDC prefers to be silent on matters that would make them take corrective action? No. Because while they commissioned the white paper under increasing pressure from the public, they also carefully chose authors who they knew would design convoluted studies incapable of answering the questions accurately, using data from the Vaccine Safety Datalink (VSD), which is only accessible by government researchers, and which lacks the ability to ascertain any child’s full and accurate status. This was step one in their plan to produce “science” to silence public concern. In contrast, Dr. Paul’s data was from children born into his practice, providing accurate data on each and every child.
Examples of Your Manufactured Charges
Your accusation that Dr. Paul solicited vaccine refusal is baffling. In reality, Dr. Paul practices medicine. His published works, his videos, and his speaking appearances very clearly show his approach to medicine. His practice has a widely known reputation for respecting fully informed consent and fully informed declinations – as required of him by Oregon law and Federal regulations. Parents seek him out because they want his style of care. To imply that he forces this on families that come to him explicitly because they know their child’s health and informed consent will be respected is absurd.
Parents that want to follow the full schedule without any information about the risks of vaccines or the opportunity for a personalized schedule to ensure minimal risk of adverse reactions for their child do not seek out Dr. Paul’s medical practice. Dr. Paul’s respect for families’ decisions not to vaccinate actually go against his financial interests – he would make far more money if he followed the same practices as his peers and worked to increase vaccination rates rather than working toward increasing good health outcomes.
All of the your charges against Dr. Paul are unsupported and malicious attempts to paint him in a bad light. Chief among these false charges is the one concerning tetanus. You stated:
“Patient D, a now 9-year-old male, was completely non-immunized. Patient D sustained a large, deep scalp laceration at home in a farm setting on August 8, 2017, and was treated with colloidal silver and with his parents suturing the wound independently. Patient D subsequently developed acute tetanus requiring intubation, tracheotomy, feeding tube placement and an almost two- month ICU stay at Doernbecher Children’s Hospital. Patient D was then transferred to Legacy Rehabilitation. Licensee saw Patient D for follow-up in clinic on November 17, 2017. Licensee’s notes documented a referral to a homeopath, recommendation of fish oil supplements, and “phosphatidyl seine(sic)” He did not document an informed consent discussion about the risk/benefit of immunization for a child who had just sustained and still had sequelae of, and remained vulnerable despite prior infection, to tetanus, a life-threatening and disabling disease that is preventable by proper vaccination. Licensee’s care placed Patient D at serious risk of harm and constitutes gross negligence.”
Someone reading the above might be led to believe that Dr. Paul had been the boy’s pediatrician throughout his childhood, including at the time he sustained the tetanus infection. Your intent appears to be to lead the public to that assumption, knowing your suspension of Dr. Paul would draw much attention. But Patient D was not Dr. Paul’s patient. Dr. Paul had never even met the child until a couple months after the child was hospitalized, and the parents were told by the hospital that they would not release the child until they had found a primary care physician to take over the boy’s care. The parents searched for an MD, but none would take their son unless they agreed to get him vaccinated. The parents steadfastly refused.
When the parents finally found Dr. Paul, he followed his oath and agreed to be the child’s doctor, respecting the parents’ medical choice against vaccination. The medical error in this case was made, unfortunately, by the parents, when they prematurely sutured the wound. Even if the boy had been vaccinated against tetanus, wounds that are not properly cleansed and treated can still lead to tetanus infections.
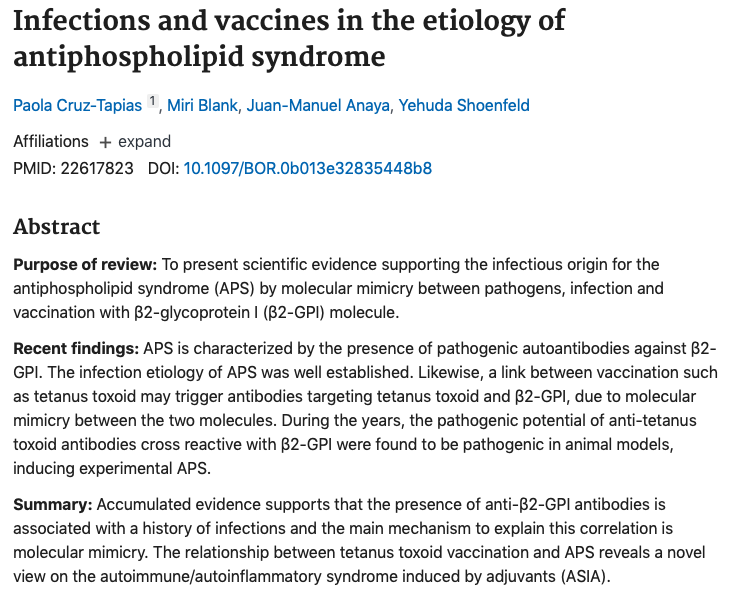
This case, ironically, also highlights the rarity of tetanus infection for the general population. The patient lived with his parents on a farm, received the wound to the head in the barn. Tetanus is caused by the bacterium Clostridium tetani, which while common in the soil, requires specific conditions to lead to infection. Tetanus is also found in the intestines of large farm animals, and so farms are potential sources of exposure, and the infection usually only becomes systemic if the wound is very deep and not properly cleansed and treated. The CDC states that prior to the introduction of the tetanus vaccine in the United States in the late 1940’s, there were just 500-600 cases reported annually, and now there are approximately 50-100. That might be a large relative risk drop, but it is a minuscule absolute risk drop. Tetanus infections went from very rare to slightly more very rare. And what about the risks of the tetanus vaccine? It used to be that individuals received just one or two doses in a lifetime. Now, because it’s in the DTaP and Tdap, and the pertussis portion of that vaccine has utterly failed, children are given six doses by the sixth grade, and women are bullied into getting a Tdap shot during every pregnancy, an off-label use pushed by the CDC that exposes developing infants to maternal immune activation and an aluminum adjuvant, a known neurotoxin. Hyper-immunization to tetanus is also a concern, as is the risk for antiphospholipid syndrome, which happens to be one of the leading causes of infertility in the U.S. today.
Another of your accusations against Dr. Paul involved screening for antibody titers to MMR. You said, “Except for rare cases of suspected immune deficiency, there is no clinical indication for assessment of antibody titers. The ordering of unnecessary testing is a violation of ORS 677.190(1)(a) unprofessional or dishonorable conduct, as defined in ORS 677.188(4)(c) willful and repeated ordering or performance of unnecessary laboratory tests.”
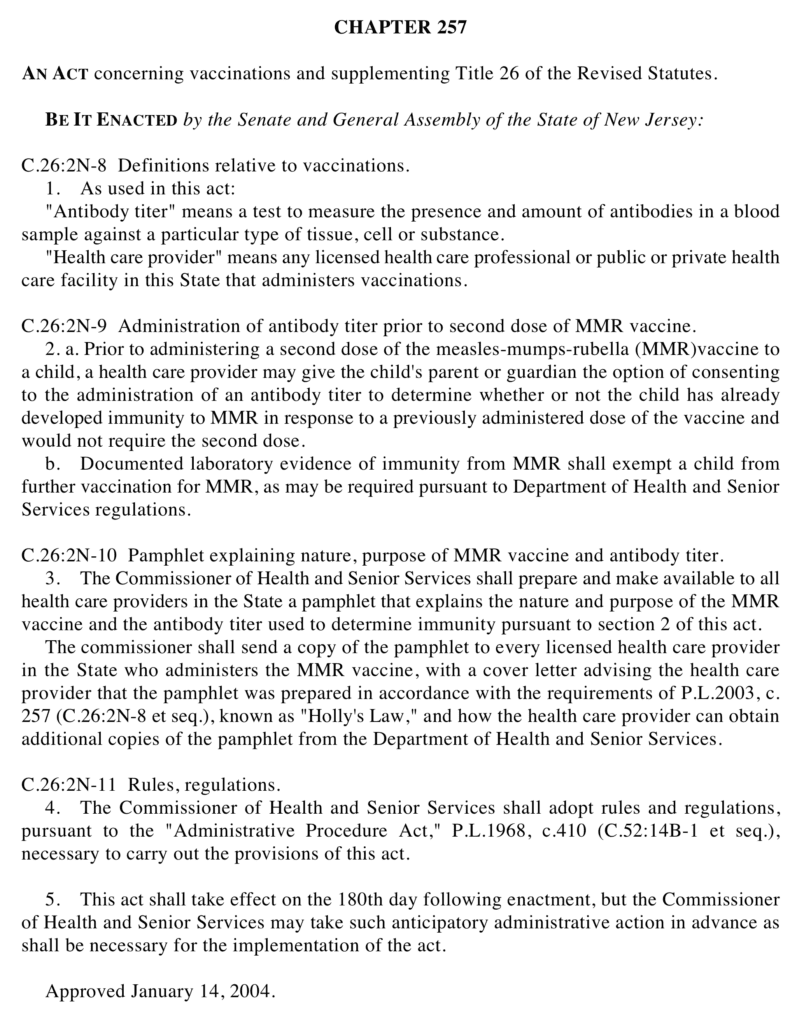
We agree that unnecessary medical procedures are universally considered a breach of medical ethics – in part because no medical procedure is without risk. But you have it all backwards. It is far safer to do a titer check on a child than to subject a child to the risks of a second dose of MMR. Oregon accepts antibody titers in lieu of receipt of a second MMR. Holly’s Law in New Jersey, named after Holly Stavola who died from a severe adverse reaction to a second dose of MMR, requires parents to be informed about the titer test option. Administering a pharmaceutical product that is not medically indicated is “unprofessional or dishonorable conduct” — titer testing rather than exposing a child to a dose that is not medically indicated is doing one’s medical due diligence. Oregon should consider passing Holly’s Law to protect ethical physicians like Dr. Paul Thomas, and you should be applauding him, not condemning.
You also quote ORS 677.265(1)(c), that states the standard of care is “that degree of care, skill and diligence that is used by ordinarily careful physicians in the same or similar circumstances in the community of the physician or a similar community.”
But you are charging Dr. Paul for exceeding the degree of care, skill, and diligence of many other practitioners. It is not a crime to go above and beyond the minimal standards — we dare say the dangerous standards — currently followed by the majority. If you are saying that the current standard of care is to treat each and every child the same, to violate the mandated Learned Intermediary duty, and to violate informed consent — then the you must immediately eliminate that standard and define a new one that upholds vaccination practices that respect the health and safety of the individual child and fully informed consent. You must abandon the product-uptake measure of a physician’s practice and adopt the health-outcome measure, for surely, you must agree that good health and not product-consumption is the goal.
You, the OMB, must also familiarize yourselves with the actual capabilities, limitations, risks, and unintended consequences of each vaccine product, including the unintended consequences of disease-symptom avoidance and vaccine-ingredient exposure, to avoid basing standards on your hopes for vaccine products rather than their reality.
You stated that Dr. Paul had published “an alternative vaccination schedule that decreases the frequency of many recommended vaccines and omits others, including rotavirus.”
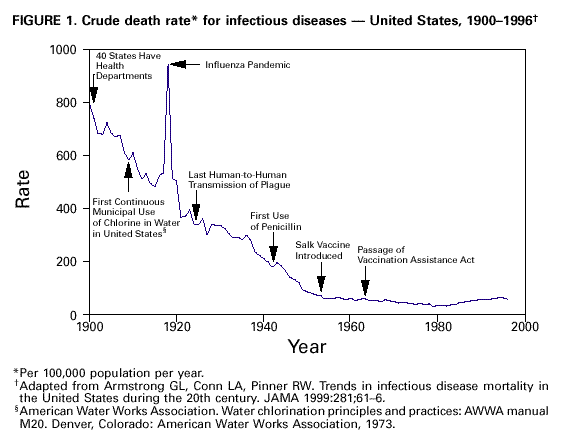
Yes, Dr. Paul’s schedule reflects his diligence to follow the full body of science on vaccine products and their impacts on children’s health. As clearly outlined in his book The Vaccine Friendly Plan, it has not been proven that the risks of the rotavirus vaccine outweigh any perceived benefit. And the growing body of science on injected aluminum should be heeded by all pediatricians, as well as the CDC, in order to First Do No Harm. Just like tetanus, before their targeting vaccines were introduced, the rates of severe outcomes and deaths due to childhood diseases, indeed all infectious diseases, had plummeted due to improved sanitation and living conditions in the U.S.
Dr. Paul’s study is showing what the CDC has avoided acknowledging: that in pushing mass vaccination without proper science on the products or the outcomes of exposure, we’ve traded experiencing transient infections and rare deaths for entire generations of children and adults experiencing chronic diseases, causing lifetimes of suffering, and premature death. Tragically, the CDC is repeating with injected aluminum its pattern of denial of harm to the public, as it did with mercury-containing thimerosal.
Surely, in 2021, medicine has advanced to the point that most severe cases of transient infections could be avoided with proper early nutrient or drug treatments. Surely we should not accept the harmful consequences of the current vaccine products, which are liability-free for their makers who highly profit off not just the sale of the vaccines but the chronic health conditions they cause. It is the very attitude of accepting the risks and collateral damage of vaccination and ignoring or censoring nutrient and drug preventives and treatments that is causing the current catastrophe we are now experiencing with SARS-COV-2 and COVID-19. We have seen systemic fraud and corruption in regards to censoring information on existing treatments, the pushing of investigational vaccines as “safe and effective” in the glaring absence of proper science on either, and this has awakened the entire world to the drug industry’s capture of public health.
As for Dr. Paul’s alternate vaccination schedule, the data speaks for itself.
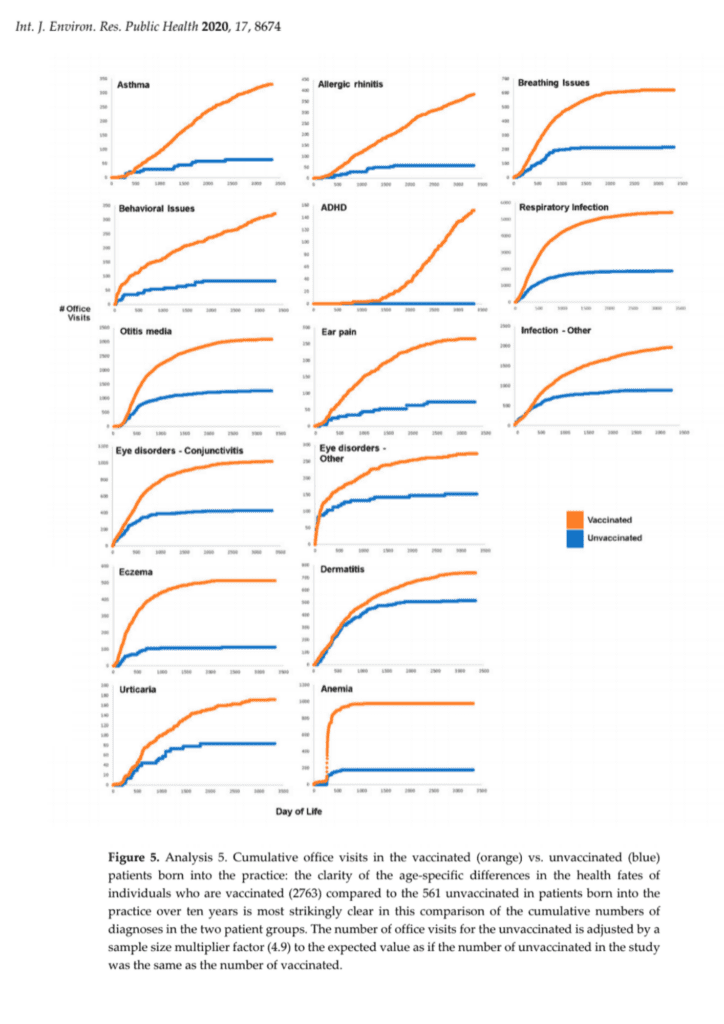
Dr. Paul, upon seeing that the fully non-vaccinated children under his care were healthier than those who followed his selective vaccination plan, has said that his Vaccine Friendly Plan is not yet friendly enough. Our question to you is, OMB, why aren’t you also comprehending that even modified schedules lead to poorer health outcomes than no vaccine exposure at all? Why isn’t this leading you to demand more similar studies, better and safer vaccine products, better science, and more accountability for health outcomes?
All vaccination comes with risk. If a child’s vaccination exposure is not personalized for that child, with all the most up-to-date information regarding both the disease to be avoided and the science on the vaccine products, then a physician is in violation of his duty toward that child.
The measure of a physician’s care should be on the health outcome of his patients, not on the volume of pharmaceutical products injected and sold or even the incidence of treatable and mostly benign vaccine-targeted disease within a practice.
You claimed that you had to immediately suspend Dr. Paul’s license because if he continued the practice of medicine, he “would pose an immediate danger to the public and to his patients.”
The facts are just the opposite. Taking Dr. Paul Thomas abruptly away from his patients is reckless and, especially for his drug-rehab patients, has put their lives at risk. To do this in the midst of a pandemic makes this action even more deplorable.
In conclusion, you, the Oregon Medical Board, must immediately reinstate Dr. Paul’s license and apologize to him, his patients, and to the entire state of Oregon for your egregious actions. You must re-examine your mission and your loyalties and take steps to eliminate the use of pharmaceutical sales quotas as “quality measures“, and you must begin to support a medical system that judges practitioners not by the number of prescriptions written but by the health of their patients.
Sincerely,