
A 2019 paper confirms acellular pertussis vaccines increase lifetime susceptibility to whooping cough.
“. . . .all children who were primed by DTaP vaccines will be more susceptible to pertussis throughout their lifetimes, and there is no easy way to decrease this increased lifetime susceptibility.”
James D Cherry; The 112-Year Odyssey of Pertussis and Pertussis Vaccines—Mistakes Made and Implications for the Future, Journal of the Pediatric Infectious Diseases Society, , piz005, https://doi.org/10.1093/jpids/piz005
Treatment
It’s important to know how to recognize potential pertussis infections, how the infection progresses, what symptoms mean, and treatment options. Always consult with your trusted medical advisor.
- “Pertussis in infants was associated with prolonged new cough (≥5 days) in infants’ household contacts. Findings suggest that breastfeeding protects against pertussis and warrants recommendation with pertussis prevention strategies, which currently include pertussis vaccination of pregnant mothers and infants’ close contacts.” PMID:28033240 This study looked at years in which birth mothers likely had received whole-cell DPT in childhood, not Tdap.
- An Italian study (PMID:27870812) looking at later years in which birth mothers were more likely to have the acellular Tdap did not find breastmilk provided adequate protection against pertussis, (but breastfeeding was still highly recommended). This may be reflective of the differing immune response between whole cell and acellular pertussis vaccines.
“Breastfeeding remains a milestone of prevention for a number of diseases, including several infectious diseases. The benefits of breastfeeding are particularly evident in low-income settings, where a number of risk factors may add to exposure to infectious diseases. Because in developed countries exclusive breastfeeding does not play a significant role in protecting unvaccinated children from pertussis, other protective strategies should be considered for preventing the disease shortly after birth. Because the impact of cocoon strategy may be hampered by asymptomatic colonization and transmission from vaccinated individuals in the households, immunization of pregnant women seems at present the most realistic strategy to prevent pertussis in young infants.”
ICWA NOTE: safety of maternal vaccination has not been established.
- VITAMIN C: Sodium ascorbate treatment of whooping cough: the alternative approach
- 19 Cases of Whooping Cough treated with Ascorbic Acid: a 1937 study published in the Canadian Medical Journal
✻ ✻ ✻ ✻
The cocooning strategy was abandoned in Australia, after an independent group evaluated it was having a negative effect.
Excerpt from a report by Toni Bark MD MHEM LEED AP with thanks to Bronwyn Hancock:
“. . . the Commonwealth Government Pharmaceutical Benefits Advisory Committee (PBAC), ‘which is totally independent and very expert, …determined that there is no clinical effectiveness’ of the cocooning strategy ‘in rotecting newborns’ from pertussis, Vic, Qld and WA also abandoned the strategy and NSW restricted and eventually abandoned it. Victoria was the only state to later revive the strategy, doing so in June 2015 only after a change of government. The PBAC’s finding appears to have been further confirmed in October 2015, when a very large Australian study (covering 64,364 live-births) was published finding that: ‘vaccinating parents with dTpa during the four weeks following delivery did not reduce pertussis diagnoses in infants.’ Medical research has found that, to the contrary, vaccination may result in ‘silent reservoirs’ of ‘readily transmitted’ infection and thus increase, instead of decrease, the risk of transmission.”
(Carcione D. et al. The impact of parental postpartum pertussis vaccination on infection in infants: A population-based study of cocooning in Western Australia. Vaccine. doi:10.1016/j.vaccine.2015.08.066 Volume 33, Issue 42, 13 October 2015, Pages 5654–5661 http://www.sciencedirect.com/science/article/pii/S0264410X15012049)
(An article in Australian Doctor magazine describes the same research:
Cocooning ineffective against pertussis. Australian Doctor. Michael Woodhead, 31 August 2015 http:// www.australiandoctor.com.au/news/latest-news/cocooning-ineffective-against-pertussis
Srugo et al. Pertussis Infection in Fully Vaccinated Children in Day-Care Centers, Israel. Emerg Infect Dis. Oct 2000;6(5). http://wwwnc.cdc.gov/eid/article/6/5/00-0512_article: “The whole-cell vaccine for pertussis is protective only against clinical disease, not against infection…. Our results indicate that children ages 5-6 years and possibly younger, ages 2-3 years, play a role as silent reservoirs in the transmission of pertussis in the community.”
Study: Is the whooping cough resurgence due to vaccinated people not knowing they’re infectious? 24 Jun 2015 BMC Medicine (http://www.santafe.edu/news/item/althouse-scarpino-whooping-cough-asymptomatic/); “
Vaccination does not prevent transmission
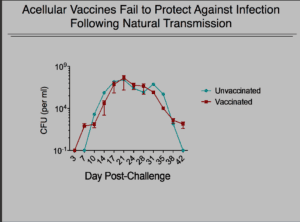
Pertussis is a very serious infection and vaccination does not prevent either colonization or transmission. In fact recent studies have shown that when exposed to pertussis (whooping cough) those who are vaccinated with the acellular pertussis vaccine are as contagious as those who are not vaccinated, only without warning symptoms to let them know they are contagious.
“Meanwhile, there was no difference in either the duration or in B. pertussis burden between unvaccinated and acellular-pertussis-vaccinated animals, while previously infected animals were not colonized following reinfection.”
Warfel JM, Zimmerman LI, Merkel TJ. 2016. Comparison of three whole-cell pertussis vaccines in the baboon model of pertussis. Clin Vaccine Immunol 23:47–54. doi:10.1128/CVI.00449-15.
From Stanley Plotkin, who has a very long career and is much respected in the world of vaccinology:
“The whole-cell pertussis vaccine that evolved in the 20th century was clearly reactogenic, although the permanence of its sequelae was exaggerated. Nevertheless, reactions were disturbing to parents and, even worse, whole-cell vaccines were extremely variable in the protection they gave, as was starkly evident in the results of the trials conducted in the 1990s, in which whole-cell vaccines were used as comparators to acellular vaccines. Specifically, whole-cell vaccines made in some European countries were shown to be much more efficacious than one made in the United States. The efficacy of vaccines made by laboratories in other parts of the world remains uncertain.
The reactions to whole-cell vaccines in high-income countries, including convulsions and hypotonic episodes, led to its rejection and replacement by acellular vaccines composed of 1–5 virulence factors of the organism. The fact that the composition of acellular vaccines has been so variable, both in the number of antigens and their concentration, testifies to the uncertainty about which factors are important, an ignorance that continues today to a certain extent. However, there was general agreement that pertussis toxin (PT), with its multiple systemic and local effects, should be included as toxoid. There was disagreement as to the need to add filamentous hemagglutinin (FHA), pertactin, and fimbria.
The situation today is that in many middle-income countries, notably in Latin America, whole-cell vaccines made by a variety of manufacturers are widely used with varying and uncertain evidence for safety and efficacy. However, in most high-income countries, including the United States, Australia, and Western Europe, acellular vaccines are the rule, but waning immunity has resulted in a resurgence of pertussis. Moreover, the tendency of low- and middle-income countries to switch to acellular pertussis vaccines has stopped in its tracks pending improvements in them. And yet, as this supplement shows, pertussis remains a problem regardless of the economic level of a country. If immunity to the infection is impermanent even after natural infection, it is even less so after vaccination. The result is the continued circulation of the bacterium in family contacts, regardless of their vaccination history, resulting in exposure of vulnerable newborns.” (emphasis added)
Plotkin, S. A. (2016, December 01). The Importance of Persistence. Retrieved December 31, 2017, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5106615/
A couple facts important to know:
- While pertussis is very serious, in Washington State, there were only 4 Pertussis deaths in 21 years from 1959 to 1980.
- Pertussis outbreaks are cyclical. During the 2012 outbreak in WA, 75.8% of cases were in fully vaccinated people who were “up-to-date” on pertussis vaccination. CDC Data.
- Other important data on the 2012 WA outbreak: “Tdap protection wanes within 2 to 4 years. Lack of long-term protection after vaccination is likely contributing to increases in pertussis among adolescents.” PMID 25941309 ; “The significant association between vaccination and isolate pertactin production suggests that the likelihood of having reported disease caused by PRN(-) compared with PRN(+) strains is greater in vaccinated persons. Additional studies are needed to assess whether vaccine effectiveness is diminished against PRN(-) strains.” PMID 25301209 ; “We investigated the molecular epidemiology of the largest pertussis epidemic in Washington State in 70 years. Given that the majority of cases were fully vaccinated, we assessed the current population of B. pertussis at a molecular level and compared the results to the current vaccine.” PMID 25031439
- This study found that during outbreaks, “At its peak, siblings were the most important sources of pertussis in infants 6 months and younger, particularly fully vaccinated children aged 2 and 3 years.” PMID 25391405
- In 2012, of the 155 reported pertussis cases in infants aged <1 year, 34 were managed in a hospital. Among these hospitalized infants, 14 were aged <2 months. Of the 2,360 cases involving children aged ≥1 year with known outcome, 14 of the children were hospitalized. No fatalities were reported.
- In the 1990’s, because DTP came with such high risk of injury, it was replaced in the U.S. with the acellular (not whole cell) DTaP and Tdap vaccines. Although capable of providing limited personal protection, these vaccines also come with risks, the protection wanes quickly, they don’t protect against mutant and emerging strains, and they cannot prevent the colonization or transmission of infection.
- Large outbreaks are occurring in fully vaccinated populations to those who have received multiple vaccine doses. Studies are showing that repeated vaccination decreases the ability to fight the infection, and mutant strains now make up 90% of pertussis infections in western countries.
- Repeated vaccination leads to the danger of hyperimmunization. This is of particular concern for the tetanus vaccine. See PMID 3499712, 8491525, 22235053, 22875539, 23238161, 25430703.
- Because of a phenomenon known as “original antigenic sin,” each subsequent vaccination with acellular pertussis vaccine makes the immune system more vaccine-strain-specific and less able to bind with wild pertussis. Lengthier infection times in those who are asymptomatic also leads to more virus mutations for which the vaccine is not protective.
- Screening and Genomic Characterization of Filamentous Hemagglutinin-Deficient Bordetella pertussis. PMID: 29358336“Despite high vaccine coverage, pertussis cases in the United States have increased over the last decade. Growing evidence suggests that disease resurgence results, in part, from genetic divergence of circulating strain populations away from vaccine references. The United States employs acellular vaccines exclusively, and current Bordetella pertussis isolates are predominantly deficient in at least one immunogen, pertactin (Prn). First detected in the United States retrospectively in a 1994 isolate, the rapid spread of Prn deficiency is likely vaccine driven, raising concerns about whether other acellular vaccine immunogens experience similar pressures, as further antigenic changes could potentially threaten vaccine efficacy. We developed an electrochemiluminescent antibody capture assay to monitor the production of the acellular vaccine immunogen filamentous hemagglutinin (Fha). Screening 722 U.S. surveillance isolates collected from 2010 to 2016 identified two that were both Prn and Fha deficient. Three additional Fha-deficient laboratory strains were also identified from a historic collection of 65 isolates dating back to 1935. Whole-genome sequencing of deficient isolates revealed putative, underlying genetic changes. Only four isolates harbored mutations to known genes involved in Fha production, highlighting the complexity of its regulation. The chromosomes of two Fha-deficient isolates included unexpected structural variation that did not appear to influence Fha production. Furthermore, insertion sequence disruption of fhaB was also detected in a previously identified pertussis toxin-deficient isolate that still produced normal levels of Fha. These results demonstrate the genetic potential for additional vaccine immunogen deficiency and underscore the importance of continued surveillance of circulating B. pertussis evolution in response to vaccine pressure.” (emphasis added)
The science on pertussis vaccines is far from settled. Public health messages claim them to be “safe and effective” and yet scientists know that the available vaccines, the diseases they aim to prevent, and the human immune system are not yet fully understood. The below abstract is from the June 2017 paper: Pertussis disease and transmission and host responses: insights from the baboon model of pertussis. https://www.ncbi.nlm.nih.gov/pubmed/28646950
Abstract
Whooping cough is a highly contagious, acute respiratory disease, caused by the Gram-negative bacterium Bordetella pertussis (Bp). Despite the introduction and widespread use of vaccines starting in the 1950s pertussis cases continue to be reported, with a significant global impact. The role of specific virulence factors in disease and the immune mechanisms associated with protection following natural infection or vaccination are still not completely understood.
During any whooping cough outbreak, government and medical agencies and the media put out messages for the community to get vaccinated. This advice provides some level of personal protection (about 70% effective against Bordetella pertussis but may be ineffective against Bordetella parapertussis) for a limited time (2-5 years is the latest guess)–but that means perhaps 30% of those vaccinated are not protected, 70% are potentially asymptomatic vectors, and waning protection in fully vaccinated populations or households means many are susceptible to infection.
Because this information is not commonly known, there is a false sense of security. Proper precautions are not being taken around newborns or the immunocompromised. Cocooning is potentially hazardous. It is a dilemma the scientific community is working hard to fix.
The CDC advises the screening of potential typical carriers during outbreaks — but such advice is insufficient to contain any outbreak. Everyone potentially exposed to pertussis needs to be tested whether or not there are symptoms present. This might seem unfeasible now, but new diagnostic technology has been developed that may make testing cost effective and fast. The developing field of RDT (rapid diagnosis technology) for pertussis and other communicable infections may provide essential tools that can be incorporated into public health measures to help limit the spread of infection.
http://www.hain-lifescience.de/en/products/microbiology/bordetella/genoquick-bordetella.html
Vaccination during pregnancy does not guarantee protection nor has it been proven safe. The FDA baboon studies found that it was possible to generate antibodies in the infant by maternal and early neonatal vaccination that proved effective in reducing or eliminating symptoms of infection when challenged, but the young baboons still colonized and transmitted infection, and the study design could not speak to safety for the human fetus or child, nor the impact of repeated vaccinations with each pregnancy, nor the long-term impact on neurological or immune health.
The FDA has not approved the pertussis vaccine–nor any vaccine–for use during pregnancy for specific protection of the infant because adequate safety studies have not been done.
“Several licensed vaccines may be used during pregnancy to prevent disease in the mother, unless specifically contraindicated, Tdap & Influenza. Vaccines recommended for pregnant women were first licensed and approved for use based on safety and effectiveness data in non-pregnant women. These vaccines were then recommended by public health policy makers for pregnant women based on their perceived benefit and minimal risk for the mother and infant. Currently, no vaccine is approved specifically for use during pregnancy to protect the infant.”
https://www.fda.gov/downloads/AboutFDA/Transparency/Basics/UCM509197.pdf
The FDA will not approve vaccines for pregnant women for protection of the infant until the appropriate studies are done, but it is repeatedly said it is unethical to run clinical trials with pregnant women because it could put the fetus in jeopardy. So why is it ethical to recommend these vaccines to pregnant women in the general population?
Pregnant women are being told that they are being given vaccines to protect the baby in language that implies, if not outright states, that appropriate safety studies have been done. They have not. Pregnant women in the general population are in essence being used in ongoing clinical trials without their fully informed consent.
Over the years, data has been gathered in a haphazard fashion using voluntary registries set up by pharmaceutical companies and in adverse event reports to VAERS, both of which suffer from extreme under-reporting. VSD (Vaccine Safety Datalink) studies on the safety of vaccination during pregnancy mostly include only pregnancies with live-birth outcomes, and very few studies look at the long-term health effects on children. One such rare study on vaccination with the influenza vaccine during pregnancy (Zerbo et al) found a significant association with autism. Even the most elaborate and inappropriate application of adjustments and corrections could not make the association go away in the first trimester, so the authors simply dismissed the result as due to chance. This is not science. http://jamanetwork.com/journals/jamapediatrics/article-abstract/2617988
The impact of maternal immune activation during pregnancy, and the impact of exposure to various vaccine components, such as the placenta-crossing 250 mcg of aluminum in the Tdap, on long-term neurological development are not known, but there’s enough science indicating that extreme caution is warranted. The current push to vaccinate during every single pregnancy, as well as during every outbreak, comes without any understanding of the health effect of such frequent administration of three disease antigens (tetanus, diphtheria, pertussis) and other vaccine components. This is a small sampling of studies on one component, aluminum:
- Multifaceted effects of aluminium in neurodegenerative diseases: A review. https://www.ncbi.nlm.nih.gov/pubmed/27479193
- Aluminum exposure and toxicity in neonates: a practical guide to halt aluminum overload in the prenatal and perinatal periods https://doi.org/10.1007/s12519-014-0477-x
- Mechanisms of aluminum adjuvant toxicity and autoimmunity in pediatric populations. https://doi.org/10.1177/0961203311430221
- Prenatal exposure to neurotoxicants and neurodevelopment in Mexican neonates. http://www.nature.com/jes/journal/v22/n4/full/jes201248a.html
- Non-linear dose-response of aluminium hydroxide adjuvant particles: Selective low dose neurotoxicity. https://www.ncbi.nlm.nih.gov/pubmed/27908630
- Association between prenatal exposure to metals and neonatal morbidity. http://www.tandfonline.com/doi/abs/10.1080/15287394.2014.932313
- There are many studies showing the neurotoxic effects of aluminum from environmental sources such as food. Only .3% of ingested aluminum is absorbed while 100% of injected aluminum is absorbed. These studies indicate the critical need for aluminum adjuvant safety research.
- Aluminum Exposure at Human Dietary Levels for 60 Days Reaches a Threshold Sufficient to Promote Memory Impairment in Rats. https://www.ncbi.nlm.nih.gov/pubmed/27473855
- In ovo toxico-teratological effects of aluminum on embryonic chick heart and vascularization https://www.ncbi.nlm.nih.gov/pubmed/27535157
- A histological study of toxic effects of aluminium sulfate on rat hippocampus. https://www.ncbi.nlm.nih.gov/pubmed/25314162
- The consequences of aluminium intake on reproductive function in male rats: a three-generation study. https://www.ncbi.nlm.nih.gov/pubmed/27513431
Pertussis is a very serious infection. Vaccination comes with risk, provides limited protection, and creates asymptomatic carriers. Safety during pregnancy has not been established. Outbreaks will continue to occur, and it’s critical that everyone be sufficiently informed of vaccination limitations and risks in order to behave in as safe a manner as possible around vulnerable populations.
Additionally, other tools must be utilized to detect those who are infected, and the safest most effective healing approaches explored in order to improve outcomes of those who become infected. It is becoming increasingly clear that pertussis is not an ideal candidate for control or eradication by vaccination.
- What Is Wrong with Pertussis Vaccine Immunity? The Problem of Waning Effectiveness of Pertussis Vaccines. PMID: 28289064
Global, federal, and state initiatives and incentives are creating enormous pressure to increase vaccination levels. None of these programs have written into their description any regard for the limitations and risks of vaccination, individual genetic or environmental susceptibility, the flexibility to incorporate new science into the plan, or any regard for medical freedom of choice. It is an undeniable fact that the entire population cannot be safely vaccinated, but protection of those at risk of injury or death from vaccination is not built into any of the programs. And in the absence of anyone being responsible for vaccine injury–from those who make vaccines, to those who administer vaccines, to health departments that promote vaccines–the messages being conveyed to the public never contain vaccine limitation and risk information critical to protecting individual health.
Science of the Dtap/Tdap/aP Vaccine
Studies cited in the above video – HERD IMMUNITY: WHOOPING COUGH
- PMID: 15304469 Association between carriage of Streptococcus pneumoniae and Staphylococcus aureus in Children.
- PMID: 18270917 Pneumococcal vaccination: conjugated vaccine induces herd immunity and reduces antibiotic resistance
- PMID: 7898220 Increase in pneumococcal bacteraemia in Sweden.
- PMID: 15361720 Changes in frequency and pathogens causing acute otitis media in 1995-2003.
- PMID: 15937758 Temporal trends of invasive disease due to Streptococcus pneumoniae among children in the intermountain west: emergence of nonvaccine serogroups
- ScienceDaily, January 28, 2011, “How bacteria keep ahead of vaccines and antibiotics.”
- PMID: 15304469 Association between carriage of Streptococcus pneumoniae and Staphylococcus aureus in Children.
- Janeway’s Immunobiology
- www.CDC.gov
- PMID: 28289058 What Is Wrong with Pertussis Vaccine Immunity? Inducing and Recalling Vaccine-Specific Immunity.
- PMID: 28289059 What Is Wrong with Pertussis Vaccine Immunity? Why Immunological Memory to Pertussis Is Failing.
- PMID: 28289064 What Is Wrong with Pertussis Vaccine Immunity? The Problem of Waning Effectiveness of Pertussis Vaccines.
- PMID: 24443545 Different effects of whole-cell and acellular vaccines on Bordetella transmission.
- PMID: 24277828 Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model.
- PMID: 10463173 Antigenic variants in Bordetella pertussis strains isolated from vaccinated and unvaccinated children.
- PMID: 19579693 A natural pertactin deficient strain of Bordetella pertussis shows improved entry in human monocyte-derived dendritic cells.
- PMID: 22914363 Appearance of Bordetella pertussis strains not expressing the vaccine antigen pertactin in Finland.
- PMID: 19751581 Bordetella pertussis strains with increased toxin production associated with pertussis resurgence.
- PMID: 24216286 Pertussis epidemic despite high levels of vaccination coverage with acellular pertussis vaccine.
- PMID: 24655754 A rapid ELISA-based method for screening Bordetella pertussis strain production of antigens included in current acellular pertussis vaccines.
- PMID: 28076445 Emerging Bordetella pertussis Strains Induce Enhanced Signaling of Human Pattern Recognition Receptors TLR2, NOD2 and Secretion of IL-10 by Dendritic Cells
- PMID: 24277828 Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model.
- INFECTIOUS BEHAVIOR: Brain Immune Connections in Autism, Schizophrenia, and Depression by Dr. Paul H. Patterson
- PMID: 28188123 The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment.
- EVERY SECOND CHILD by Dr. Archie Kalokerinos
- PMID: 24325827 Co-administration of live measles and yellow fever vaccines and inactivated pentavalent vaccines is associated with increased mortality compared with measles and yellow fever vaccines only. An observational study from Guinea-Bissau.
- PMID: 21691704 In vivo study of hepatitis B vaccine effects on inflammation and metabolism gene expression.
- PMID: 15626943 Hepatitis B vaccination associated with higher female than male mortality in Guinea-bissau: an observational study.
- PMID: 7975851 Suboptimal response following intradermal hepatitis B vaccine in infants.
- PMID: 24570246 Live vaccine against measles, mumps, and rubella and the risk of hospital admissions for nontargeted infections.
- PMID: 27840013 Simultaneous Vaccination with MMR and DTaP-IPV-Hib and rate of hospital admissions with any infections: A nationwide register based cohort study
- Federal Register, DHHS, FDA 1984, Vol. 49, No. 107
- Pertussis carrier: http://www.fda.gov/…/Newsr…/PressAnnouncements/ucm376937.htm
- Diphtheria carrier: http://www.cdc.gov/diphtheria/clinicians.html
- Pertussis epidemic despite high levels of vaccination coverage with acellular pertussis vaccine. http://www.ncbi.nlm.nih.gov/m/pubmed/24216286/
- “Further, we show that aP vaccination impedes host immunity against B. parapertussis-measured as reduced lung inflammatory and neutrophil responses. Thus, we conclude that aP vaccination interferes with the optimal clearance of B. parapertussis and enhances the performance of this pathogen. Our data raise the possibility that widespread aP vaccination can create hosts more susceptible to B. parapertussis infection.” http://www.ncbi.nlm.nih.gov/m/pubmed/20200027/
- “Our unvaccinated and under-vaccinated population did not appear to contribute significantly to the increased rate of clinical pertussis. Surprisingly, the highest incidence of disease was among previously vaccinated children in the eight to twelve year age group.” http://www.ncbi.nlm.nih.gov/pubmed/22423127
- Vaccinations create more powerful and virulent strains of bacteria and viruses. The reason for the current whooping cough outbreak. Read more here from the CDC “Vaccination against 2 avian viruses, the Marek disease virus, and the infectious bursal disease virus, were associated with the emergence of more virulent strains (33). An important role of host immunity in selecting for virulence is also suggested by the co-evolution of the myxomatosis virus and rabbits (34). Furthermore, immune pressure was shown to select for more virulent Plasmodium chabaudi parasites in mice (35). Based on mathematical modeling, vaccines designed to reduce pathogen growth rate and/or toxicity may result in the evolution of pathogens with higher levels of virulence. http://wwwnc.cdc.gov/eid/article/15/8/08-1511_article.htm
- “After the fifth dose of DTaP, the odds of acquiring pertussis increased by an average of 42% per year.” http://www.nejm.org/doi/full/10.1056/NEJMoa1200850…
- This study shows that efficacy of the DTaP falls rapidly. At 2 years post-vaccination, it’s just 75%. By 5 years, it’s down to 11.9%. http://www.ncbi.nlm.nih.gov/pubmed/24903664
- Pertussis 53 – 64% effective in adolescents and adults: http://www.ncbi.nlm.nih.gov/pubmed/23873919
- Tetanus is anaerobic, so it dies when it hits oxygen. Bleeding from an injury is a good thing. Tetanus is more common where farm animal feces is present. If tetanus is suspected, an immune globulin shot can be administered. Getting a tetanus shot at the time of injury is a moot point. It would take several weeks to create antibodies, and if tetanus were present, death could occur within a week. Tetanus is extremely rare. Severe tetanus in immunized patients with high anti-tetanus titers. https://www.ncbi.nlm.nih.gov/m/pubmed/1565228/
- Adverse event reports after tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccines in pregnant women. https://www.ncbi.nlm.nih.gov/m/pubmed/22727350/
Risks of Dtap/TDap (beyond vaccine failure)
- The Dtap/TDap vaccine is associated with the most adverse reactions recorded (VAERS database.)
- See Aluminum and Mitochondria pages
- this section under construction
If after exploring this page you’d like the State of Washington to take immediate action to address the pertussis dilemma, please sign this PETITION.
Disclaimer